Nearly 65% of dental practices participate with dental insurance, which means the majority of offices must navigate insurance billing regularly. With 50.2% of the adult population in the United States utilizing dental insurance, the volume of claims is significant. Yet many practices experience revenue loss from missed billing processes. Annually, the average dental practice loses 9% of collectible revenue to missed dental billing processes. A structured approach to billing can help capture this lost income.
Defining Dental Billing and Its Core Components
Dental billing refers to generating medical claims to submit to insurance companies for reimbursement for oral health services. It has two parts: patient billing and insurance claims processing. Patient billing involves collecting patient balances, co-pays, and deductibles. Insurance claims processing involves preparing, submitting, and tracking claims to third-party payers.
The work is often handled by dental assistants, dedicated billing staff, or outsourced partners. A dental assistant may collect insurance information and send bills to insurance companies, but specialized billers bring deeper expertise in codes, payer policies, and appeals. Skilled human oversight remains critical, even as artificial intelligence tools improve accuracy and consistency in claim processing.
The Two Sides of Dental Billing
Insurance billing and patient billing operate together. The insurance side focuses on verifying benefits before treatment, submitting clean claims, and following up on unpaid balances. The patient side handles statements, payment plans, and communication about out-of-pocket costs.
Understanding which party owes what is essential. After the insurance carrier pays its portion, the patient becomes responsible for the remaining balance. If the claim is denied or underpaid, the practice must decide whether to appeal or bill the patient depending on the policy terms.
AR management– Monitoring accounts receivable and pursuing unpaid claims.
Patient billing – Generating statements and collecting patient balances.
Timing is crucial. Insurance claims should be submitted within one to two business days of treatment. If a claim remains unpaid after two to three weeks, the practice should begin the appeal process. In most states, insurance companies must pay claims within 30 to 45 days, so tracking deadlines is important.
These numbers show that most practices rely on insurance reimbursement, and even small errors can accumulate into significant revenue loss over time.
Important Distinctions in Dental Billing
One critical distinction is between participating and non-participating dentists. Participating dentists agree to accept the insurance carrier’s allowed amount as full payment and cannot balance-bill the patient beyond that amount. Non-participating dentists may bill up to their full fee, and the patient is responsible for any difference between the fee and what the insurance pays. Participating dentists should always check with the carrier for allowed amounts before billing.
Another distinction involves Medicare. To bill Medicare for covered dental services, a provider must be Medicare-enrolled. While Medicare generally does not cover routine dental care, certain medically necessary services may qualify, and enrollment is required to submit claims.
Clear billing practices help practices avoid compliance issues and maintain healthy patient relationships. Whether billing in-house or partnering with a specialized firm, understanding these basics is the foundation of a financially stable dental practice.
What is the difference between dental billing and dental coding?
Dental coding involves assigning standardized CDT codes to procedures performed. Dental billing uses those codes to prepare and submit insurance claims. Coding must happen accurately before billing can proceed. Both functions rely on each other to ensure payment.
How long does an insurance company have to pay a dental claim?
In most states, insurance companies must pay claims within 30 to 45 days. If a claim is not paid within that window, the practice should follow up with the payer. The exact timeline can vary by state law and individual carrier policies.
Can a dental assistant handle insurance billing?
Yes. Dental assistants may collect insurance information and send bills to insurance companies. However, complex billing tasks such as appeals, coordination of benefits, and medical cross-coding often require dedicated billing expertise or outsourced support.
What happens if a claim is denied?
If a claim is unpaid after two to three weeks, the practice should begin the appeal process. The first step is to review the denial reason, gather supporting documentation, and resubmit or appeal according to the carrier’s guidelines. Persistence and accuracy are key to getting paid.
The American Dental Association estimates that as many as 30 percent of dental practices experience some form of employee theft or embezzlement. For a practice generating $1 million in annual revenue, a typical embezzlement scheme can drain $50,000 to $100,000 or more before detection. That is lost profit, lost investment, and lost trust. Preventing embezzlement in dentistry requires more than a basic accounting check. It demands deliberate financial oversight, strong internal controls, and a willingness to challenge the assumption that “my staff wouldn’t do that.” Implementing effective dental practice embezzlement prevention strategies is crucial.
Control Area
What It Prevents
Implementation Example
Segregation of duties
Cash skimming, fake adjustments
One person posts payments, another person reconciles daily deposits
Daily reconciliation
Missing deposits, unposted payments
Compare daily schedule to payment log and bank deposit
Approval for adjustments
Unauthorized write-offs
All adjustments over $25 require a second signature or owner approval
Periodic audits
Undetected long-term theft
Quarterly review of adjustment reports and delinquent accounts
Electronic payment systems
Cash handling risk
Encourage credit cards and EFT payments to reduce cash exposure
Implementing these controls does not require an expensive accounting department. Even a small practice can adopt simple checks:
Have the practice owner open mailed checks and stamp them “for deposit only.”
Require all cash payments to be recorded immediately on a numbered receipt.
Compare the daily appointment schedule to the day’s payment log every afternoon.
Run a monthly report of all adjustments and review each one for legitimacy.
Surprise the team with an occasional midday cash drawer count.
These steps take minutes per day but create a visible deterrent. Staff members who know checks are in place are far less likely to test the system.
The Role of Practice Management and Financial Oversight
Strong practice management goes beyond scheduling and insurance verification. It includes active financial oversight from the owner or an outside partner. Many dentists feel uncomfortable scrutinizing staff, but that hesitation allows theft to continue. A better approach is to frame internal controls as protecting both the practice and the employees. When everyone knows that checks exist, temptation decreases.
Financial oversight should include monthly revenue cycle reviews. Look for red flags such as:
An increase in adjustments or write-offs
A rise in the number of delinquent accounts
Cash payments that seem low compared to appointment volume
A staff member who refuses to take time off
Ledger entries that lack supporting notes or documentation
One practice owner discovered a $70,000 loss only after noticing that the office manager had not taken a single vacation day in three years. A mandatory two-week absence revealed manipulated deposit records that had been ongoing for over a year. If you lack the bandwidth for this level of monitoring, consider partnering with a firm that offers revenue cycle management services.
Leveraging Professional Dental Accounting and Audits
Dental accounting specialists understand the unique revenue patterns of a dental practice. A professional audit can uncover irregularities that a general accountant might miss. For instance, an unusually high number of “courtesy adjustments” or duplicate entries in patient ledgers can signal employee theft dental activities. Regular audits are one of the most effective embezzlement prevention tips available.
A comprehensive dental billing audit services review examines:
Payment posting accuracy
Adjustment and refund reports
Outstanding accounts receivable
Deposit timeliness
Insurance claim submission patterns
An outside firm can provide an objective perspective. When practice owners conduct their own audits, they may subconsciously overlook patterns that would be obvious to an impartial reviewer. A specialized dental auditor knows exactly which reports to pull and what ratios indicate manipulation. They can flag a sudden spike in courtesy adjustments or a pattern of small cash write-offs that would not draw a practice owner’s attention.
Embezzlement Prevention Tips for Practice Owners
Here are actionable steps you can take today to reduce the risk of dental fraud in your practice:
Separate financial duties. Never let one person handle all steps of payment from receipt to deposit to reconciliation.
Use lockbox or electronic payment services. Reducing cash transactions lowers exposure. Encourage patients to pay by card or through EFT payments for dental practices.
Review monthly reports personally. Spend 30 minutes each month scanning adjustments, refunds, and transaction logs. Look for patterns, not just totals.
Conduct surprise cash counts. Occasionally count the petty cash drawer or deposit bag and compare to recorded amounts.
Trust your gut but verify. If something feels off, investigate. Many owners later admit they sensed something was wrong but did not follow through.
Bring in an outside auditor annually. A third-party audit adds a layer of deterrence and detection. The cost is small compared to a six-figure loss.
Practice security also involves safeguarding patient data. Embezzlement often begins with access to patient accounts and insurance information. Limit system permissions to the minimum needed for each role. Do not give every staff member full administrative access to practice management software. Create user roles that match job responsibilities and require manager approval for privilege escalation.
When to Seek Expert Help: How Outsourced Billing Adds Security
One of the most powerful embezzlement prevention strategies is removing financial duties from in-house staff altogether. By outsourcing insurance billing and payment posting to a specialized partner, you eliminate the opportunity for internal theft in those functions.
Outsourced dental billing providers like Steadfast Billing Solutions act as an independent check on your practice’s revenue. They process claims, post payments, and reconcile accounts without the emotional relationships that can lead to collusion or oversight gaps. Additionally, their expertise in dental accounting and insurance claims reduces the chance that errors or omissions go unnoticed.
For practices that have already experienced employee theft dental issues, outsourcing can restore trust and stabilize cash flow. The combination of internal controls for cash handling at the front desk and outsourced processing for insurance and patient billing creates a strong barrier against embezzlement in dentistry. Even practices that have never experienced theft benefit from the separation of duties outsourcing provides, because it splits the revenue process across two independent organizations with no personal loyalty to each other’s staff.
Frequently Asked Questions
How common is embezzlement in dental practices?
Studies suggest that 20 to 30 percent of dental practices will experience embezzlement at some point. The median loss exceeds $60,000, and many cases go undetected for more than two years.
What are the early signs of dental office theft?
Common red flags include a staff member who rarely takes vacation, cash payments that seem low, adjustments that look unusual, or a sudden increase in patient accounts with no explanation. Comparing daily logs to deposits can reveal discrepancies.
Can a small practice afford strong internal controls?
Yes. Basic controls like segregation of duties, daily reconciliation, and monthly financial reviews cost nothing but a small time investment. For practices that want an extra layer, outsourcing billing is a cost-effective solution.
How does outsourcing billing help prevent embezzlement?
Outsourcing removes payment processing and claims handling from in-house staff, eliminating the opportunity for internal theft in those areas. An external team provides independent financial oversight and expert auditing that can catch irregularities early.
What should a practice owner do if they suspect theft?
Gather evidence quietly before confronting anyone. Run reports showing adjustments, refunds, and daily deposit records. Compare payment logs to bank statements. Contact a dental accountant or attorney who specializes in practice fraud. Do not tip off the suspected employee until you have documented proof and a plan for how to proceed.
Do bonding or insurance policies cover embezzlement losses?
Some practice insurance policies include a crime or fidelity bond that covers employee theft. Check your policy language. Standard general liability policies usually do not cover embezzlement. A separate crime policy or a fidelity bond can reimburse part of the loss, though prevention remains the better approach.
Incorporating dental practice embezzlement prevention measures can create a more secure financial environment for your practice.
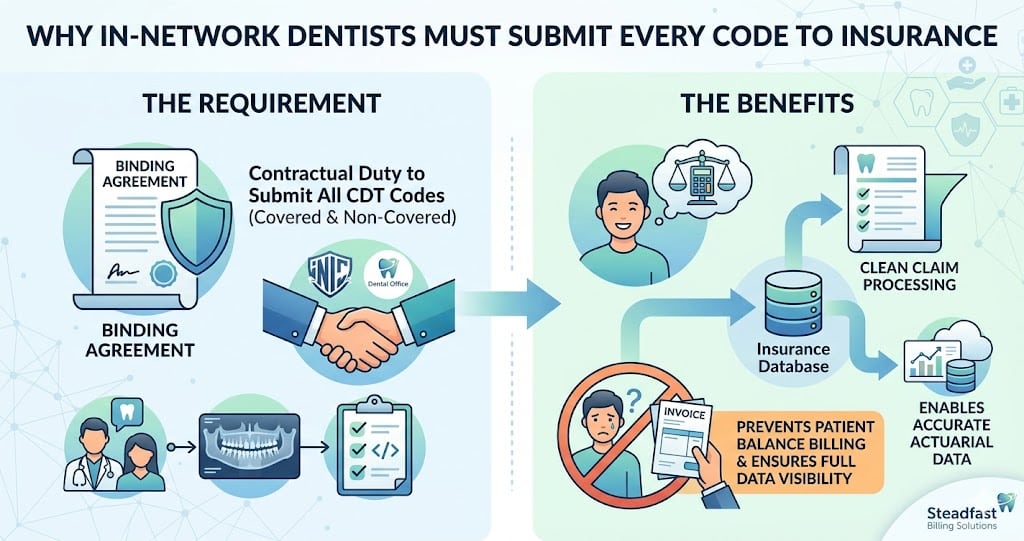
When a practice signs an in-network contract with an insurance carrier, the agreement comes with a clear mandate: an in-network dentist must submit every code to insurance as they must report every procedure performed, regardless of whether the plan covers that specific service. This obligation, rooted in both the contract and federal regulations, protects patients from surprise bills and ensures carriers have full visibility into treatment patterns. Yet many dental offices misinterpret the requirement, either omitting non-covered codes or billing patients directly for services that should first pass through the carrier. The consequences range from clawbacks and contract termination to compliance audits. Insurance carriers increasingly use automated systems to cross-reference clinical notes with submitted codes, making omissions easy to detect.
Misunderstanding full code submission requirements can cost a practice tens of thousands of dollars annually in clawbacks and lost revenue. The following sections examine the contractual language, common pitfalls around CDT code submission, and practical steps to remain compliant while maximizing legitimate revenue.
Why an In-Network Dentist Must Submit Every Code to Insurance Under Contract
Every participating provider agreement contains a provision stating that the in-network provider requirements include the submission of all charges for services rendered to an insured patient. Insurance companies phrase this as a “clean claim” obligation, but the definition extends beyond formatting. The true requirement is that the dental claim processing system receives every CDT code that accurately describes the procedure, even if the code is considered non-covered or not eligible under the patient’s benefit plan.
Failure to follow this protocol constitutes a breach of contract. Carriers routinely audit claims histories and cross-reference patient records. When they discover that a provider omitted a code, they may demand repayment for all related services and sometimes terminate the provider agreement entirely. For a practice that relies on a steady flow of in-network patients, that risk is existential.
The logic behind the rule is straightforward: insurance companies price their premiums and networks based on actuarial data. If they only see partial data from providers, their pricing models become inaccurate. They also want to prevent balance billing scenarios where a patient receives a service, the provider submits only covered codes, and then the patient receives a separate bill for the unsubmitted service. That practice, called “disentangling,” violates most state insurance regulations.
Where Practices Commonly Go Wrong with Code Submission
The most frequent error occurs when a dentist performs a procedure that the plan categorizes as a non-covered benefit. For example, a panoramic X-ray for orthodontic evaluation or a surgical extraction that the plan excludes. The team, trying to be helpful, might skip submitting that code because “the insurance won’t pay anyway.” This is a violation. The contract requires submission of all codes, not just payable ones.
In many policies, non-covered benefits still apply toward a patient’s deductible or maximum. When omitted, the patient may unknowingly be billed at a higher out-of-pocket rate than they should. And if the carrier discovers the omission during an audit, they can recalculate the entire claim and demand a refund.
Using Incorrect CDT Codes to Fit a Patient’s Plan
Some billers change a CDT code to a different one that is more likely to be paid, rather than submitting the true code. This practice, known as “denial avoidance,” is a form of insurance fraud. Even if the intention is to help the patient, using a code that does not describe the actual procedure violates both dental coding guidelines and the provider contract. Accurate code submission is not optional.
Skipping Pre-Authorization as a Workaround
Dental pre-authorization may not be required for every procedure, but when a carrier requests it, the submission of the planned codes during the pre-auth step is separate from the claim itself. Some practices assume that if pre-authorization was denied, they do not need to submit the claim. They are incorrect. The in-network contract demands claim submission regardless of prior denial. The carrier needs the claim to formally process the denial and to track the patient’s benefits.
The Role of the Dental Fee Schedule in Submission Compliance
The dental fee schedule that accompanies an in-network contract establishes the maximum allowable fee for each CDT code. When a practice submits all codes, the carrier applies the fee schedule and calculates the patient’s copayment and the carrier’s payment. If a code is omitted, the fee schedule for that code is never triggered, and the patient may be left with a balance that should have been covered.
Insurance claim codes must always be submitted with the full billed charge, even if the fee schedule will reduce it. Carriers expect to see the practice’s usual fee, not an arbitrary amount. Submitting a reduced fee to avoid a contract violation is itself a misrepresentation. The correct approach is to submit the true usual and customary fee, then let the fee schedule do its work.
How Insurance Claim Processing Checks for Compliance
Carriers use automated edit engines to flag claims where a provider consistently omits certain codes. For example, if a practice performs a high volume of oral surgery procedures but never submits adjacent diagnostic codes like D024 (intraoral occlusal film), the system may trigger a review. Similarly, if a provider’s claim submission patterns change abruptly or deviate significantly from peer profiles, an investigation begins.
During an audit, the carrier compares the submitted claims against clinical notes, radiographs, and treatment plans. Any missing codes become evidence of non-compliance. The penalties can include recoupment of payments for all affected patients, monetary fines, and exclusion from the network.
Practices often underestimate how sophisticated cost analysis tools have become. Carriers now have access to artificial intelligence that can predict expected code combinations based on the procedure and tooth number. A routine filling on tooth 19 without a diagnostic code or bitewing radiograph in the same visit automatically triggers a compliance check. The margin for error is thin.
Practical Steps for In-Network Dentists to Ensure Full Code Submission
Build a Standardized Clinical Documentation Checklist
Every clinical note must list every procedure performed, including diagnostic exams, radiographs, anesthetic administration (D9210 series), and adjunctive services. The front desk or billing team should code directly from this checklist, never from memory or habit. This reduces the chance of overlooking a routine code like D9120 (removal of restoration) that often goes unsubmitted.
Use a Clearinghouse That Validates Code Completeness
A clearinghouse is more than a pass-through. Many modern clearinghouses offer real-time edits that flag claims where the code bundle appears incomplete relative to the procedure. For example, if you submit a crown code D2740 without a preliminary code for the buildup or the core, the clearinghouse can raise an alert. Integrating these checks into the dental claim processing workflow catches omissions before the carrier sees them.
Train Staff on Insurance Billing Protocols
The administrative team must understand that their duty is to submit every code without editorial judgment. A helpful but misguided staff member who decides “the insurance won’t pay for this so I’ll save the patient a denial letter” is actually creating liability. Regular training sessions on insurance billing protocols should reinforce that submission is contractually required, not optional.
Periodic audits performed by a third party can reveal patterns of omission that have become routine. An audit reviews a sample of claims against the clinical records and identifies any codes that were not submitted. Even a small practice can benefit from a quarterly review. For practices that lack the staff time, outsourcing to a dental billing audit service ensures impartial scrutiny and documented compliance.
When Full Submission Conflicts with Patient Communication
A natural tension arises when a patient asks, “Why are you billing my insurance for something they won’t cover?” The answer is simple: the contract requires it. But patients may perceive it as wasteful or intrusive. The practice should prepare a brief explanation: “Our agreement with your insurance company requires us to report every service we provide. This helps them maintain accurate records of your benefits and ensures that anything that does count toward your deductible is tracked properly.”
This scripting empowers the front desk to address concerns without getting into clinical details. It also positions the practice as a stickler for compliance, which builds trust.
Full code submission becomes even more critical when a patient has dual coverage. If only one carrier receives all codes while the second receives a partial list, the coordination of benefits process breaks down. The secondary carrier may underpay or deny benefits because they lack the full picture. Accurate submission to both carriers is essential for proper coordination of benefits, a topic we cover in depth in our article on [link: coordinating multiple insurance plans].
Missing codes also complicate the resolution of termed coverage. When a patient’s policy has ended but services were rendered while active, the carrier may require a complete code list to finalize the account. Incomplete submissions delay resolution and can lead to balance confusion for the patient.
Table: In-Network vs. Out-of-Network Code Submission Requirements
Requirement
In-Network Provider
Out-of-Network Provider
Must submit every code performed
Yes, contractually required
Not required, but recommended for patient benefit tracking
Accept fee schedule reduction
Yes
No; patient pays the difference
Balance billing restricted
Yes; cannot bill patient above allowed amount
Allowed, within state limits
Pre-authorization often mandatory
Many plans require it
Usually not required
Carrier audits for completeness
Frequent and aggressive
Rare
Penalties for omitted codes
Recoupment, contract termination
Reduced payment, possible network exclusion if joining later
How Steadfast Billing Solutions Supports Compliance
For practices that find the compliance burden too heavy to manage alongside patient care, partnering with an expert billing firm offers a clean solution. Steadfast Billing Solutions acts as an extension of your administrative team, ensuring that every claim submitted meets carrier requirements and that no code falls through the cracks. Our team lives inside the nuances of dental coding guidelines and in-network provider requirements. We do not process claims in a silo; we audit each submission against the clinical record and the contract terms.
Our dental insurance billing services include a detailed review of every fee schedule to confirm that the correct code set has been applied. We also manage dental claim processing from start to finish, including the retrieval of EOBs and the follow-up on any late payments. By outsourcing this function, your practice gains confidence that your submission practices are bulletproof.
We also offer a dental revenue cycle management approach that looks at the entire financial picture, not just claim submission. This includes dental pre-authorization follow-up, patient billing for non-covered services, and termed coverage resolution. Our goal is to make sure that the contractual requirement to submit all codes does not become a source of lost revenue or audit risk.
Frequently Asked Questions
What happens if an in-network dentist does not submit all codes to insurance?
The insurance company may require the practice to refund payments for related services, impose fines, or terminate the provider agreement. Repeated violations can lead to exclusion from the network entirely, which significantly reduces patient volume.
Does submitting a code for a non-covered service waste the patient’s time?
No. Even for non-covered services, the code must be submitted because it applies to the patient’s deductible and annual maximum. Also, some plans later apply a non-covered benefit to the out-of-pocket cap. Submitting ensures accurate benefit tracking.
Can a practice charge the patient directly instead of submitting a non-covered code to insurance?
No. Under most in-network contracts, the practice must submit all charges to the carrier first. Only after the carrier processes the claim and either pays or denies it can the practice bill the patient for any patient-responsible amount.
How often should a practice audit its claim submission compliance?
At least quarterly. More frequent audits are advisable for high-volume practices or those that have recently joined new networks. An audit can identify patterns of omission before they trigger a carrier investigation.
What are the consequences of using an incorrect CDT code to avoid a denial?
Using an incorrect CDT code is considered insurance fraud, even if no monetary loss occurs. Carriers and regulators view this as a serious compliance failure that can lead to recoupment, civil penalties, and legal action. Always submit the code that accurately describes the procedure performed.
Conclusion
The requirement that an in-network dentist submit every code to insurance is not a suggestion but a binding contractual duty. Practices that treat this obligation as optional expose themselves to audits, clawbacks, and potential network exclusion. By building robust documentation workflows, training staff on compliance, and leveraging expert support from a firm like Steadfast Billing Solutions, you can meet this requirement without sacrificing efficiency or profitability. The safest path is to submit every code, every time, and let the carrier process it as the contract dictates. Your practice, your patients, and your bottom line will benefit from that discipline.
A dental practice’s average claim denial rate hovers near 15%, directly draining tens of thousands of dollars in potential revenue each year. This persistent leakage isn’t just about insurance company policies; it’s often a symptom of an overburdened internal system. This is where specialized dental billing services shift from a cost line to a critical profit center.
These services manage the entire financial backbone of a practice, from the initial patient call to the final payment posting. They bring precision to dental coding, tenacity to follow-up, and deep expertise in payer rules that most front-office teams simply cannot match while also managing patient care.
The Core Functions of a Professional Dental Billing Service
A full-service billing partner does far more than just submit claims. They act as an extension of your practice’s administrative team, handling the intricate, time-consuming processes that determine cash flow.
Pre-Treatment: Verification and Eligibility
The financial process begins before the patient is even seated. Effective insurance verification confirms coverage levels, benefit maximums, and specific plan limitations. This step prevents surprises for both the practice and the patient, allowing for accurate financial consultations and reducing the risk of non-payment.
Treatment Day: Accurate Coding and Claim Creation
This is where clinical work meets financial protocol. Specialists translate procedure notes into the correct Current Dental Terminology (CDT) codes. A single coding error, like confusing D7953 with D7950 for bone grafts, can trigger an immediate denial. Experienced billers ensure each claim submission is narratively and technically perfect, supported by the required documentation like a precise dental excision claim narrative.
Post-Submission: Vigilant Follow-Up and Management
After submission, the work intensifies. Services track claims daily, respond to payer requests, and appeal denials with clinical and contractual justification. They actively manage the practice’s accounts receivable, focusing on aging claims to accelerate dental reimbursement. This persistent follow-up is what transforms submitted claims into collected revenue.
The Tangible Benefits of Outsourcing Your Billing
Partnering with a dedicated service yields measurable improvements that affect both your practice’s finances and its daily operations.
First, collections increase. With experts focused solely on maximizing reimbursements, practices often see a 5-15% lift in net collections. Denials drop sharply because claims are coded correctly the first time and followed up on systematically. This leads to faster payment cycles and improved cash flow predictability.
Second, internal efficiency soars. Your team is freed from the frustrating cycle of claim status checks and payer phone calls. They can redirect their energy toward patient care, scheduling, and other front-office duties that enhance the patient experience. This can reduce staff burnout and turnover related to billing stress.
Finally, you gain expertise and compliance peace of mind. Dental billing regulations and payer policies change constantly. A professional service stays current on these changes, ensuring your practice remains compliant and adapts its processes proactively, mitigating audit risk. For example, the 2024 CDT code update introduced several new codes for adjunctive procedures; a dedicated billing service would have implemented these changes immediately to prevent claim rejections.
Dental Billing Services vs. In-House Management: A Clear Comparison
Choosing between an in-house team and an external partner is a significant decision. The right choice depends on your practice’s size, volume, and internal resources. This comparison highlights the key differences.
Consideration
In-House Billing Team
Professional Dental Billing Service
Expertise Depth
Limited to staff training & experience; high turnover risk.
Deep, specialized knowledge across all payers and complex cases.
Technology & Software
Practice bears full cost of billing software, updates, and security.
Service provides advanced, dedicated billing platforms at no extra cost.
Operational Cost
Salary, benefits, training, and overhead for full-time employees.
Predictable percentage-based or flat fee; scales with production.
Focus & Productivity
Staff split between billing, front desk, and patient duties.
100% dedicated to revenue cycle management and collections.
Denial Management
Often reactive; denials can stack up due to time constraints.
Proactive tracking and aggressive appeal processes standard.
Integrating a Billing Service into Your Practice Workflow
A smooth transition is critical for success. The best dental billing services will guide you through a structured onboarding process. This begins with a comprehensive audit of your current accounts receivable and past claim data to identify leakage points.
Clear communication protocols are then established. Most services use secure, cloud-based platforms where your team can upload treatment notes and superbills daily, and where you can monitor real-time reports on collections, denial rates, and A/R aging. Regular performance reviews, often monthly or quarterly, ensure the partnership stays aligned with your practice’s financial goals. For a deeper look at the transition process, consider the insights on dental billing outsourcing versus expanding your front desk team at dental billing outsourcing.
Key Features to Look for in a Billing Partner
Not all services are created equal. When evaluating a potential partner for your dental claims processing, prioritize these non-negotiable features.
First, look for transparent reporting. You should have 24/7 access to a dashboard showing key performance indicators like net collection rate, days in A/R, and clean claim submission rate. Second, ensure they offer dedicated specialists, not a generic call center. Your practice should have a direct point of contact who understands your specific needs.
Third, verify their technology stack supports seamless electronic claims submission and secure, HIPAA-compliant data exchange with your practice management software. Finally, assess their approach to problem-solving. Ask how they handle complex coordination of benefits scenarios or challenging denials. Their answers will reveal their true expertise. A service that excels in these areas forms the core of effective dental revenue cycle management.
The Direct Impact on Your Practice’s Financial Health
The ultimate measure of any dental billing service is its effect on your bottom line. Beyond just increasing collections, a proficient partner improves financial stability. Predictable cash flow allows for better budgeting and investment in new technology or staff. Reduced accounts receivable aging means your money is working for you sooner.
Furthermore, the cost savings are substantial. When you factor in the salaries, benefits, software licenses, and continued training for a qualified in-house biller or team, the fixed fee of a service often proves more economical. This converts a variable, management-heavy cost into a predictable operating expense. To understand the full scope of this financial impact, reviewing a breakdown of current average dental claim denial rates can be enlightening dental claim denial rates.
Taking the Next Step for Your Practice
The complexity of dental insurance billing will only increase. Relying on an overstretched front office team to manage it is a strategic risk to your revenue. Professional dental billing services provide the specialization, technology, and relentless focus needed to close revenue gaps permanently. They turn your practice’s financial operations from a source of stress into a streamlined, profit-optimizing engine. The first move is an objective assessment of your current revenue cycle performance to identify specific areas for improvement. From there, you can explore how a dedicated partner aligns with your practice’s growth goals, perhaps starting with a focused look at enhancing your dental insurance claims managementdental insurance claims management.
Frequently asked questions
How much do dental billing services cost?
Most services charge a percentage of collections, typically between 5% and 9%. Some offer flat-fee structures per claim or a monthly rate. The model depends on practice size and claim volume. The key is to evaluate the net increase in collections against the fee to assess true ROI.
Will I lose control over my finances if I outsource billing?
No, you gain more control through superior data. Reputable services provide real-time, transparent dashboards showing all financial metrics. You retain full ownership of your funds and bank accounts; the service manages the process of securing payments from insurance companies on your behalf.
How long does it take to transition to an outsourced service?
A full transition typically takes 30 to 90 days. This includes an initial audit, system integration, training, and the phased transfer of active accounts receivable. A good service manages this process with minimal disruption to your daily cash flow.
Can a billing service handle specialty dentistry claims?
Yes, a top-tier service will have coders and specialists experienced in periodontics, endodontics, oral surgery, and orthodontics. They understand the unique narratives, documentation, and coding requirements for complex procedures, which is essential for maximizing dental reimbursement in specialty fields.
What happens to my current accounts receivable when I switch?
A professional service will conduct a detailed audit of your existing A/R and develop a plan to work these aging claims. They will either take over the entire backlog immediately or work it down systematically alongside new claims, ensuring no revenue is left behind during the transition.
Oral surgeons send over 30% of their major claims to medical insurers. Yet, a high number are denied or underpaid. This happens because of incorrect coding. This is not just a small error. It is a revenue leak that costs a practice thousands of dollars each year. Medical cross coding for oral surgery procedures changes dental CDT codes into medical CPT or ICD-10 codes. This helps medical plans see and pay your claims. Learning this change is vital for surgical offices. It ensures you get full pay for medical care. Every office should create a dental procedure cross-reference sheet to make this easy.
Why Your Practice Needs Accurate Cross Coding
Many oral surgery procedures are not purely dental. Treatments for sleep apnea, facial trauma, pathological lesions, reconstructive surgery, and complex implant placements often have clear medical diagnoses and implications. Most dental software uses CDT codes. However, medical payers use CPT and ICD-10 codes. This difference often leads to denied claims. This disconnect is where revenue disappears. Effective dental-medical integration hinges on a correct dental to medical code translation. Failing to map the procedure correctly results in instant denials for “non-covered service” or downcoding to a less reimbursable, non-surgical code.
A successful claim hinges on more than just the procedure code. It requires a robust clinical narrative that justifies medical necessity, linking the ICD-10 diagnosis code to the chosen CPT surgical code. This process of procedure code mapping and narrative building is a specialized skill. It’s one reason many practices partner with a dedicated dental insurance billing services provider who understands both clinical and coding requirements.
There is no simple, one-to-one dictionary for converting CDT to CPT codes. This dental crosswalk is based on the clinical substance of the procedure, not its name. For example, a single surgical service might be described in the CDT manual, but its medical counterpart could be defined by anatomical location, surgical approach, and time complexity in the CPT manual. This surgical coding conversion requires clinical knowledge.
Consider bone grafting. CDT code D7953 (bone replacement graft – first site) describes the procedure dentally. For medical billing, the correct CPT code could range from 21210 (graft to maxilla) to 21215 (graft to mandible), or even codes for obtaining the graft itself (20900-20902). Choosing incorrectly can trigger audits or underpayment. A detailed resource like our essential guide to bone graft codes can help clarify these complex scenarios. According to a 2022 survey by the American Association of Oral and Maxillofacial Surgeons, practices using structured crosswalk resources reduced bone grafting claim denials by an average of 40%.
Common Oral Surgery Coding Scenarios and Medical Crosswalks
Here is a simplified reference table for common oral surgery procedures, illustrating the conceptual shift from dental to medical coding. This table underscores why generic code translation software often fails.
Used when removal involves bone removal, sectioning, or is for a medical diagnosis like osteomyelitis.
Excision of Benign Lesion
D7465
40810, 41116 (Excision of lesion)
CPT code is determined by exact anatomical location (vestibule, floor of mouth, etc.) and size.
Frenectomy
D7960
40819 (Frenectomy)
One of the rarer direct correlations, but medical diagnosis (e.g., speech impediment) is still required.
Treatment of Facial Fracture
D7999 (Unspecified)
21310-21497 series
CPT is exquisitely specific to the bone fractured (mandible, zygoma, orbital floor) and treatment type (open vs. closed).
How to Use Cross-Coding in Your Office
Standardizing your approach to oral surgery coding is critical for consistency and compliance. Follow these steps to build a reliable system.
Establish Medical Necessity First: Before considering codes, document a clear medical diagnosis (e.g., obstructive sleep apnea, infection, trauma, congenital defect) that justifies the procedure beyond dental health.
Perform the Code Translation: Use authoritative resources like the American Medical Association’s CPT manual and ADA’s CDT manual together. Don’t rely on memory or outdated spreadsheets. This is the heart of medical cross coding for oral surgery procedures.
Craft a Powerful Claim Narrative: The narrative tells the story the codes cannot. It should succinctly connect the patient’s symptoms, medical diagnosis, and the medical rationale for the specific surgical technique used. For complex cases like tumor excision, a well-written dental excision claim narrative is indispensable for approval.
Verify Payer-Specific Rules: Some medical plans have unique policies or preferred codes for oral surgery. Always check the patient’s medical plan benefits and guidelines before submission.
Even with perfect coding, claims can be entangled by secondary payers. A firm grasp of coordination of benefits strategies is essential to navigate which insurer pays first and how to collect the remaining balance. For instance, a patient with both medical and dental coverage for an implant following cancer resection requires a specific submission sequence to maximize reimbursement.
Inaccurate cross coding has direct and severe financial consequences. The most immediate is claim denial, which halts cash flow and triggers costly rework. Under a typical dental revenue cycle management system, a denied claim must be investigated, corrected, and resubmitted, adding administrative costs. Worse, persistent coding errors can trigger payer audits, leading to demands for repayment of previously collected funds and potential fines.
Many practices unknowingly undercode, selecting a simpler, lower-reimbursement CPT code because the mapping seems safer. This leaves significant money on the table for every major surgery. Conversely, overcoding or using an unlisted code without proper justification can be construed as fraud. The financial stability provided by expert medical billing for oral surgery lies in accurately capturing the full value and complexity of the surgical service provided. A single mis-coded orthognathic surgery case, for example, can represent a loss of $5,000 to $15,000 in unrecovered revenue.
Optimizing Your Billing for Surgical Success
Given the complexity, many oral surgery practices find that managing this process in-house diverts excessive staff time from patient care and still yields suboptimal results. The specialized knowledge required for consistent success makes dental billing outsourcing a strategic consideration. A specialized partner brings dedicated expertise in cross-coding guidelines, stays current with annual CPT and ICD-10 updates, and has systems to track and appeal denials effectively.
This allows your clinical team to focus on surgery while ensuring your billing department, whether in-house or outsourced, functions as a precision engine for revenue capture. The goal is to transform your billing from a cost center into a reliable, optimized stream of revenue that fully reflects the medical caliber of your surgical work. One multi-surgeon practice in Texas reported a 22% increase in net medical collections within nine months of implementing a dedicated cross-coding protocol with their outsourced team.
When should I use medical cross coding for an oral surgery procedure?
Use medical cross coding when the procedure addresses a health condition beyond the teeth and supporting structures. Key indicators include treatment for trauma, infection, obstructive sleep apnea, congenital defects, or pathological lesions. If the primary diagnosis is medical, the claim typically belongs on the medical insurance.
How do I choose between an unlisted CPT code and a specific one?
Always use a specific, defined CPT code if one accurately describes the procedure. Use an unlisted procedure code (like 41899) only when no existing CPT code matches the service performed. With unlisted codes, a detailed operative report and strong medical necessity narrative are absolutely mandatory for payment.
Do all medical payers accept claims for oral surgery procedures?
No, coverage varies significantly by plan. While most are required to cover medically necessary procedures, exclusions exist. It is crucial to verify benefits and obtain pre-authorization for major surgeries whenever possible. Never assume a medical plan will cover a procedure simply because it was performed by an oral surgeon.
What is the biggest mistake practices make with cross coding?
The most common mistake is using a dental CDT code on a medical claim form. Medical payers do not recognize CDT codes. This guarantees a denial. The second biggest mistake is weak documentation that fails to establish a clear link between the patient’s medical diagnosis and the specific surgical procedure billed.
How often do coding guidelines change?
CPT codes are updated annually by the American Medical Association, and ICD-10 codes are updated each October by the CDC. CDT codes are also revised yearly. Failing to implement these updates can immediately invalidate your claims. Regular coder education is non-negotiable for maintaining compliance and revenue integrity.
Dental practices consistently lose between 5% and 15% of their annual revenue to billing errors and inefficient processes. A free dental billing audit is the most direct method to identify these leaks before they drain your profitability. This no-cost examination of your billing systems provides a clear snapshot of your revenue cycle health without financial commitment. It reveals specific, actionable issues that may be costing you thousands each month.
What Exactly is a Free Dental Billing Audit?
A free dental billing audit is a comprehensive, complimentary review of your practice’s billing procedures, claims submission, and payment posting. It is not a superficial glance. Experts analyze a sample of your claims and accounts receivable data to pinpoint errors in coding, documentation, and insurance follow-up. This process serves as a diagnostic tool, offering a detailed report on your practice’s financial vulnerabilities. Many providers offer this as an introductory service to demonstrate their expertise and the potential value of a ongoing partnership. It is a risk-free dental practice billing assessment.
This complimentary dental billing review focuses on real data from your practice. Analysts look for patterns in denials, underpayments, and aging accounts. They check for compliance with current payer rules and correct application of CDT codes. The goal is to provide you with a factual basis for improving your revenue cycle, not just a list of problems. For a deeper understanding of common pitfalls, explore our guide on dental claim denial rates.
Key Areas Examined in a No-Cost Audit
A thorough audit systematically reviews the entire claims lifecycle to find weak points.
1. Dental Claims Analysis and Error Checking
The core of the audit is a free dental claims analysis. Auditors scrutinize submitted claims for clerical errors, incorrect patient data, and mismatched procedure codes. They verify that the claim narrative supports the code used and that all required attachments are present. A simple dental billing error check here can uncover issues like duplicate submissions or claims sent to the wrong insurer. These mistakes directly cause delays and denials.
2. Coding Compliance and Insurance Protocols
Coding is a major source of revenue loss. A no cost dental coding audit ensures that procedures are billed with the most accurate and specific CDT codes. Auditors assess whether your coding maximizes legitimate reimbursement and adheres to payer-specific policies. This segment also functions as a free dental insurance audit, reviewing how well your team handles coordination of benefits, verifies eligibility, and appeals denied claims. Proper management of these areas is crucial for clean claims.
3. The Full Revenue Cycle and Accounts Receivable
The audit extends beyond initial submission. A free dental revenue cycle audit evaluates the efficiency of your payment posting, denial management, and patient collection processes. It includes a free dental ar analysis to examine the age and status of your outstanding accounts. Are there consistent delays from certain insurers? Is your team effectively following up on underpayments? This holistic view identifies bottlenecks that slow your cash flow.
Audit Focus Area
Common Issues Found
Potential Impact
Claims Submission
Incorrect patient IDs, missing narratives
Instant claim denial
Procedure Coding
Upcoding, undercoding, outdated codes
Rejected claims or audits from payers
Payment Posting
Misapplied payments, unposted adjustments
Inaccurate financial reporting
Accounts Receivable
Aging claims over 90 days, lack of follow-up
Significant cash flow disruption
Each of these areas contributes to your practice’s overall financial health. A dental billing compliance review ensures your operations meet industry standards and reduce legal risk. For instance, a 2024 survey by the American Dental Association found that 40% of practices with high denial rates had never conducted a formal billing audit, highlighting a common oversight.
The Direct Benefits to Your Dental Practice
Investing time in a free audit yields substantial returns. The primary benefit is financial clarity. You receive a report detailing exactly where money is being left on the table. This allows you to make targeted corrections that immediately improve collections. For example, fixing a single recurring coding error can recover lost revenue across dozens of future claims.
Operational efficiency is another major gain. The audit often reveals process gaps that burden your staff. Streamlining these steps through better dental insurance claims management frees your team to focus on patient care. It also reduces the stress and time spent on claim reworks and angry patient calls about billing issues.
Finally, the audit provides a benchmark for future performance. It sets a baseline from which you can measure improvement. This is invaluable for planning growth or considering dental billing outsourcing. Knowing your starting point helps you make informed decisions about resource allocation. A practice in Ohio, after its audit, reallocated 10 hours of administrative work per week to patient engagement, directly increasing case acceptance by 15%.
How to Get Started with Your Free Dental Billing Audit
Initiating a free dental billing audit is straightforward. Most reputable billing companies offer this service with no obligation. The process typically begins with a signed business associate agreement to protect patient data. You then provide secure access to a sample of your claims data, often from the last 60-90 days. The auditing team analyzes this information and schedules a review call to present their findings.
Prepare for this conversation by having your key staff available. Discuss the audit report openly, asking questions about the root causes of identified issues. The final report should include prioritized recommendations, such as staff training on specific codes or implementing new software checks. Your next step is to create an action plan based on these insights. For practices looking to address all identified gaps, comprehensive dental billing audit services offer a structured path forward.
What information do I need to provide for a free dental billing audit?
You will typically provide a sample of de-identified claim forms, explanation of benefits statements, and accounts receivable aging reports. The auditor needs enough data to spot patterns, usually 30-50 claims across different payers and procedure types.
How long does a complimentary dental billing review take?
From data submission to final report, the process usually takes 10 to 14 business days. The timeline depends on the complexity of your practice and the volume of records provided for analysis.
Will this audit disrupt our daily operations?
No. A well-conducted audit is minimally invasive. Your team may need to spend a small amount of time gathering records, but the analysis happens externally. There is no interruption to your billing or patient care workflows.
What happens after the free audit?
You receive a detailed report with findings and recommendations. The choice is yours. You can implement changes internally, seek further consulting, or engage the company for ongoing billing management. There is no pressure to purchase additional services.
Can an audit really improve my cash flow?
Yes. By identifying and correcting systematic errors, you reduce claim denials and speed up payments. Even small fixes, like improving claim narratives, can have a dramatic effect on your practice’s monthly collections and overall financial stability. One pediatric dental practice reported a 22% reduction in accounts receivable over 60 days old within three months of implementing audit recommendations.
Achieving peak dental AI front office efficiency is no longer a luxury; it is a necessity for modern practices. As we move further into 2026, the gap between tech-forward offices and those relying on manual entry is widening. At Steadfast Billing Solutions, we have seen firsthand how the right balance of automation and human expertise can transform a struggling revenue cycle into a streamlined engine. This guide breaks down exactly what you need to know to stay ahead of the curve.
Technology is moving faster than ever in the dental industry. From 3D printing to digital impressions, clinical tech has transformed patient care. However, the biggest shift is currently happening in the front office. Many practices are asking if artificial intelligence is a legitimate solution or just another marketing buzzword.
When we talk about dental AI front office efficiency, we have to separate the hype from the reality. Is AI coming for your job? No. Is it coming to make your job significantly easier? Absolutely.
The true power of AI lies in its ability to handle repetitive, high-volume tasks that often lead to human error. At Steadfast Billing Solutions, we believe in using technology to sharpen our precision without losing our “boutique” level of service.
AI shines in three specific areas:
Predictive Claim Scrubbing: Technology can now scan thousands of claims to find missing attachments or incorrect codes before they ever reach the clearinghouse.
Insurance Verification: Automated tools can pull benefit breakdowns in seconds, which allows your team to focus on the patient sitting in front of them instead of staying on hold with insurance companies.
Data Trends: AI can spot patterns in denials from specific payers, which helps us pivot our strategy faster than a manual audit ever could.
The Hype: What AI Cannot Do
Despite the flashy advertisements, there are things technology simply cannot replace. A boutique billing experience requires a level of nuance that an algorithm hasn’t mastered yet.
While AI can help with appeals, it cannot handle complex clinical appeals. It doesn’t understand the unique relationship between a dentist and a long-time patient. Most importantly, AI lacks the empathy required to discuss financial arrangements for a major treatment plan. If you rely solely on automation, you risk losing the personal touch that defines a high-end practice.
Balancing Tech and the Boutique Touch
Efficiency shouldn’t come at the cost of your practice’s culture. We use advanced systems to ensure your Dental Revenue Cycle Management is airtight, but our human experts are always the ones driving the ship.
By automating the “busy work,” your front office staff can return to being “patient coordinators” rather than “data entry clerks.” This shift is the secret to true dental AI front office efficiency. It creates a environment where your team is happier and your collections are higher.
Improving Your Practice Valuation Through Tech
Implementing the right technology isn’t just about daily ease; it is about the long-term health of your business. When a practice demonstrates high dental AI front office efficiency, it becomes more attractive to potential buyers or partners. Clean data, faster turnaround times on claims, and reduced overhead all contribute to a higher practice appraisal. By integrating these tools now, you are building a legacy of accuracy and profitability that lasts well beyond the current billing cycle.
Is Your Practice Ready to Level Up?
If you feel like your front office is drowning in paperwork despite having the latest software, it might be time for a new approach. Combining cutting-edge technology with specialized expertise is how you truly scale.
Understanding the latest D4346 dental billing guidelines is essential for practices that want to bridge the clinical gap between a standard prophy and SRP.
For years, dental hygiene coding felt like a binary choice: either the patient was “healthy” (D1110) or they had “bone loss” (D4341/D4342). This left a massive clinical gap for patients with heavy inflammation but no attachment loss.
Enter D4346. While it has been around for several years, it remains one of the most underutilized, and frequently denied, codes in the hygiene department.
Decoding the Differences: D4346 Dental Billing Guidelines & Framework
Understanding exactly where D4346 sits in the hierarchy is the first step to avoiding “downcoding” by insurance carriers.
Code
Definition
Clinical Presentation
D1110
Prophylaxis (Preventive)
Healthy tissue or slight gingivitis. Focus is on prevention.
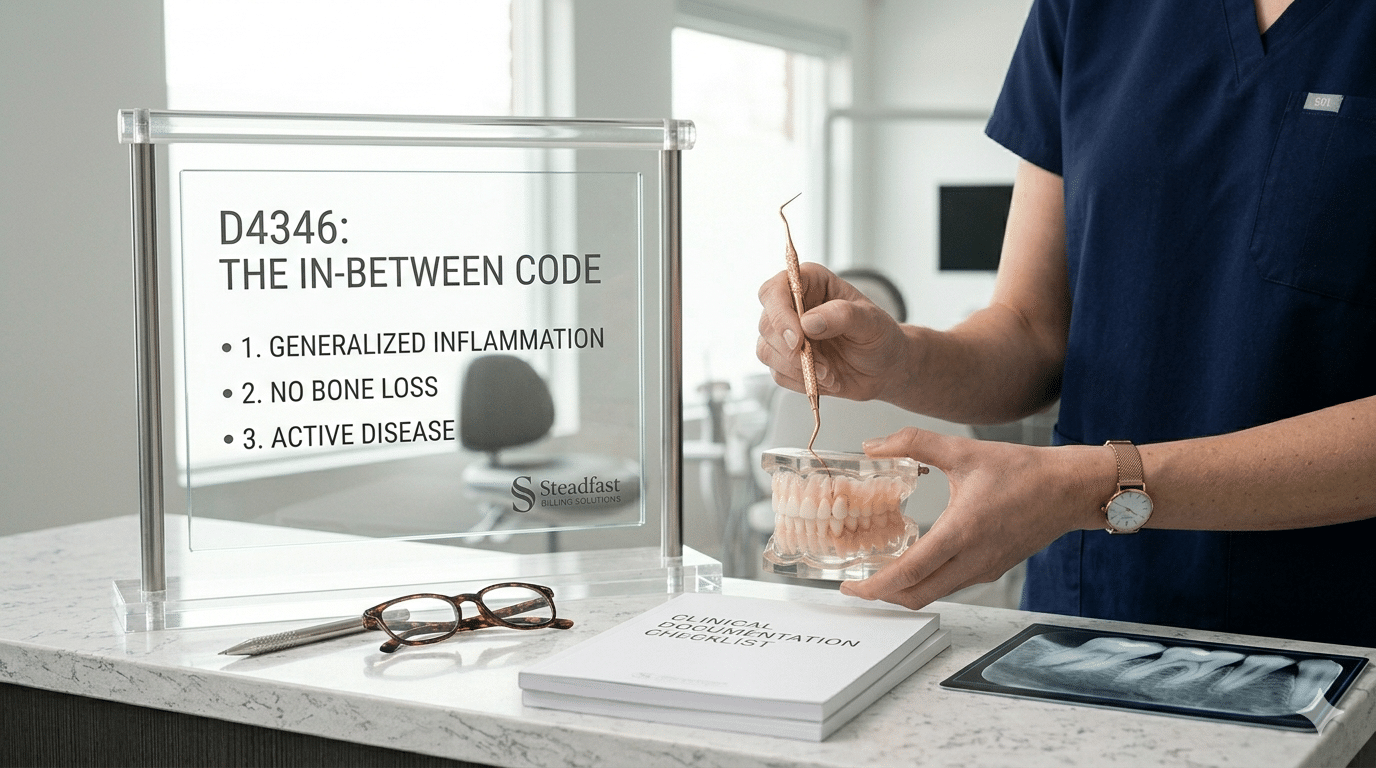
D4346
Scaling in Presence of Inflammation
Moderate-to-severe gingivitis without bone loss. Focus is on therapeutic treatment.
D4341/D4342
Scaling & Root Planing (SRP)
Active Periodontitis with bone loss and attachment loss.
The Critical Distinction
The most common mistake is trying to bill D4346 for a “bloody prophy.” However, D4346 is not a preventive code; it is a therapeutic one. Unlike a prophy, it is performed after a diagnosis of generalized moderate or severe gingival inflammation.
D4346 Documentation Requirements: Meeting the 2026 Standards & Proving Medical Necessity
To mitigate the risk of denials, your clinical records must act as a roadmap that leads the payor to one inevitable conclusion: D4346 is the only appropriate treatment. It is no longer enough to simply state a patient has gingivitis; you must provide “clinical proof” of an active disease process.
Your claim should be supported by:
Comprehensive Periodontal Charting: A complete record of the mouth that serves as the foundation for your diagnosis.
Detailed Inflammation Metrics: Clear documentation of Bleeding on Probing (BOP) scores and specific notes on the severity of the inflammation.
The 30% Threshold: To meet the criteria for “generalized” inflammation, your charting must demonstrate that moderate-to-severe inflammation affects at least 30% of the patient’s teeth.
Sulcus Depth Verification: Accurate pocket depths—generally 4mm or less—to confirm the absence of periodontitis.
Confirmation of Stability: Definitive evidence that there is no radiographic bone loss or clinical attachment loss (CAL).
The “Active Disease” Narrative: Clinical notes documenting the presence of plaque and calculus alongside generalized inflammation across multiple quadrants. Your notes should explicitly discuss the transition from health to an active disease state.
Diagnostic Radiographs: Current, high-quality X-rays that demonstrate perfectly intact bone support.
Visual Evidence:Intraoral photographs are the gold standard for D4346. High-resolution images showing red, bulbous, or “shiny” inflamed tissue provide the visual “why” that data alone sometimes misses.
3. The Narrative (The Story)
One of the most frequent questions we hear at Steadfast Billing is, ‘Why is D4346 being denied?’ Often, it’s because the practice isn’t following the specific guidelines required by 2026 payors.
When moving from a prophy to a more intensive treatment, your gingivitis billing code strategy must change. Understanding how to appeal D4346 denials starts long before the claim is sent—it starts in the hygiene chair with the right D4346 clinical narrative sample
A strong narrative prevents a “robotic” denial. Don’t just list the code; describe the clinical necessity.
Sample Narrative:“Patient presents with generalized moderate-to-severe gingival inflammation (45% BOP) in the absence of attachment loss or bone loss. Scaling in the presence of inflammation (D4346) is required to treat active gingival disease and return the patient to a state of oral health.”
Best Practices for Your Hygiene Workflow
Code for the Disease, Not the Coverage: Never let a patient’s “prophy-only” insurance dictate the clinical diagnosis. If the patient has 40% bleeding and no bone loss, D4346 is the correct clinical code.
The “Follow-Up” Appointment: Most experts recommend a follow-up “evaluation” or D1110 several weeks later to see how the tissue responded. Check your specific payor contracts for frequency limitations on these combinations.
Stop Leaving Hygiene Revenue on the Table
Optimizing your dental hygiene coding isn’t just about one claim; it’s a vital part of your overall dental revenue cycle management. At Steadfast Billing, we focus on dental insurance optimization to ensure your practice is rewarded for the clinical excellence you provide.
How do I explain the difference between a Prophy and D4346 to a patient?
The best way to explain it is to focus on the diagnosis. “A prophy is like a professional cleaning for healthy gums to keep them that way. Today, however, your gums are showing signs of active infection and significant inflammation. We are performing D4346 to treat that infection and prevent it from turning into permanent bone loss.”
Can I bill D4346 if the patient has 4mm pockets?
Yes, as long as there is no bone loss or clinical attachment loss. D4346 is often the perfect code for the “pseudo-pocket” (swollen tissue that creates a 4mm reading) where no actual recession or bone destruction has occurred.
What if the insurance company downcodes D4346 to a D1110?
This usually happens because the documentation didn’t clearly show that the inflammation was “generalized” (across 30% or more of the mouth). If you have intraoral photos and a clear BOP (Bleeding on Probing) percentage, you have strong grounds for an appeal.
Is there a waiting period between D4346 and the next Prophy?
Most payors allow a D1110 (Prophylaxis) at the next 6-month interval once the tissue has returned to health. However, some clinical protocols suggest a 2–6 week follow-up evaluation. Always check specific carrier frequency limitations to avoid unexpected patient balances.
Does D4346 require a prior authorization?
Generally, no. Because it is a therapeutic treatment for an active condition, it is typically billed after the service. However, having your “Documentation Checklist” (photos, charting, and radiographs) ready for the claim submission is vital to preventing a request for additional information (RFI).
What is the D4346 “30% Rule” I keep hearing about?
To qualify for D4346, the moderate-to-severe inflammation must be generalized. In coding terms, this means it must affect more than 30% of the teeth present in the mouth. If the inflammation is localized to only a few teeth, a D1110 is usually still the appropriate code.
Managing dental patient credit balances is one of the most overlooked aspects of dental billing, yet it is incredibly common for offices to be holding $20,000 or more in these funds. While it might look like a safety net on your aging report, those funds don’t actually belong to the practice, and holding onto them too long can lead to serious legal headaches.
Many practices struggle with dental patient credit balances because the ledger cleanup process feels overwhelming.
The Law of the Land: Refund or Relinquish
Many teams assume that if a patient doesn’t ask for their money back, the office can just keep those dental patient credit balances. This is a misconception. Unless you have a signed note or digital record stating the patient has explicitly requested to leave the credit on their account for future services, you are legally obligated to return those funds within a specific timeframe.
What If You Can’t Find the Patient?
If a patient has moved or changed their contact information, your job isn’t over. You are required to make a “good faith attempt” to reach them. If those attempts fail and these dental patient credit balances remain unclaimed past your state’s ‘dormancy period,’ you cannot simply pocket the money. past your state’s “dormancy period,” you cannot simply pocket the money or write it off.
At that point, you are required by law to submit the funds to your State Treasury as unclaimed property (a process known as escheatment).
Most states require you to attempt a refund to the patient within 30 to 60 days of identifying an overpayment. If the patient cannot be reached, the “Dormancy Period” begins. Once that period ends, you are legally required to report the dental patient credit balances to the state as unclaimed property.
Cleaning your ledgers today saves your sale price tomorrow!
Best Practices for Your Office
To keep your dental patient credit balances from becoming a liability:
Monthly Audits: Run a credit balance report at least once month.
Immediate Refunds: If a patient is done with treatment and has a credit over $5, send the check immediately.
Document Everything: If a patient wants to keep a credit for their next cleaning, get it in writing.
Holding onto patient credits isn’t just bad accounting. It’s a compliance risk. Clean up those ledgers today to protect your practice and your reputation!
The Hidden Deal-Breaker: How Credits Hurt Your Practice Sale
If you are planning to sell your practice, whether next year or ten years from now, your credit balances will be under a microscope. During due diligence, a savvy buyer’s CPA or transition consultant will scrutinize your aging reports.
Here is why high patient credit balances are a “red flag” for buyers:
It’s a Legal Liability: Buyers don’t want to inherit a practice that has potential legal “escheatment” issues (failure to report unclaimed property). They may view $30k in credits as a $30k debt they now owe.
It Lowers the Purchase Price: Often, a buyer will demand that the total credit balance be deducted from the final sale price. Essentially, you lose that money twice. Once when you didn’t collect it correctly, and again when it’s taken out of your practice’s valuation.
It Signals Operational Risk: A ledger stuffed with credits suggests that the front office systems are unorganized. If a buyer sees $20k in “unresolved” money, they wonder what else is slipping through the cracks? Denied claims, unposted adjustments, or poor clinical notes?
Asset vs. Debt: To a lender, credits are a “debt” on the balance sheet. This can complicate the buyer’s ability to secure financing if the practice’s liabilities appear too high.
The Bottom Line: A “clean” ledger with minimal credits makes your practice much more attractive and “turnkey” for a buyer. Cleaning up your credits now ensures you aren’t leaving money on the table when it’s time to exit.
Used by Google Analytics to determine which links on a page are being clicked
30 seconds
__utmx
Used to determine whether a user is included in an A / B or Multivariate test.
18 months
_ga_
ID used to identify users
2 years
_gat
Used to monitor number of Google Analytics server requests when using Google Tag Manager
1 minute
_ga
ID used to identify users
2 years
_gid
ID used to identify users for 24 hours after last activity
24 hours
__utmv
Contains custom information set by the web developer via the _setCustomVar method in Google Analytics. This cookie is updated every time new data is sent to the Google Analytics server.
2 years after last activity
__utmz
Contains information about the traffic source or campaign that directed user to the website. The cookie is set when the GA.js javascript is loaded and updated when data is sent to the Google Anaytics server
6 months after last activity
__utmb
Used to distinguish new sessions and visits. This cookie is set when the GA.js javascript library is loaded and there is no existing __utmb cookie. The cookie is updated every time data is sent to the Google Analytics server.
30 minutes after last activity
__utmc
Used only with old Urchin versions of Google Analytics and not with GA.js. Was used to distinguish between new sessions and visits at the end of a session.
End of session (browser)
__utma
ID used to identify users and sessions
2 years after last activity
__utmt
Used to monitor number of Google Analytics server requests
10 minutes
_gac_
Contains information related to marketing campaigns of the user. These are shared with Google AdWords / Google Ads when the Google Ads and Google Analytics accounts are linked together.
90 days
Marketing cookies are used to follow visitors to websites. The intention is to show ads that are relevant and engaging to the individual user.
LinkedIn Insight is a web analytics service that tracks and reports website traffic.